
America is finally ready to admit that age matters, even when it comes to our physician workforce. Here’s why I’m worried that our nation’s physicians are getting too old.

As a patriot, I watched the swift descent of President Biden’s re-election campaign with a mix of fascination and horror. Now in early 2025, we are all aware of how that turned out.
After decades of denial, it seems that America is finally ready to admit that age matters. In fact, when surveyed in mid 2024, most Americans thought that both Biden and Trump were too old for another term. This is presumably a big factor that eventually led to President Biden stepping aside for Vice President Harris. (Little good that did!)
Never before has the age of our governmental leaders been on such public display. In addition to the concerns over Biden, striking examples of age related lapses in leaders like Senators Mitch McConnell and the late Diane Feinstein were widely reported.
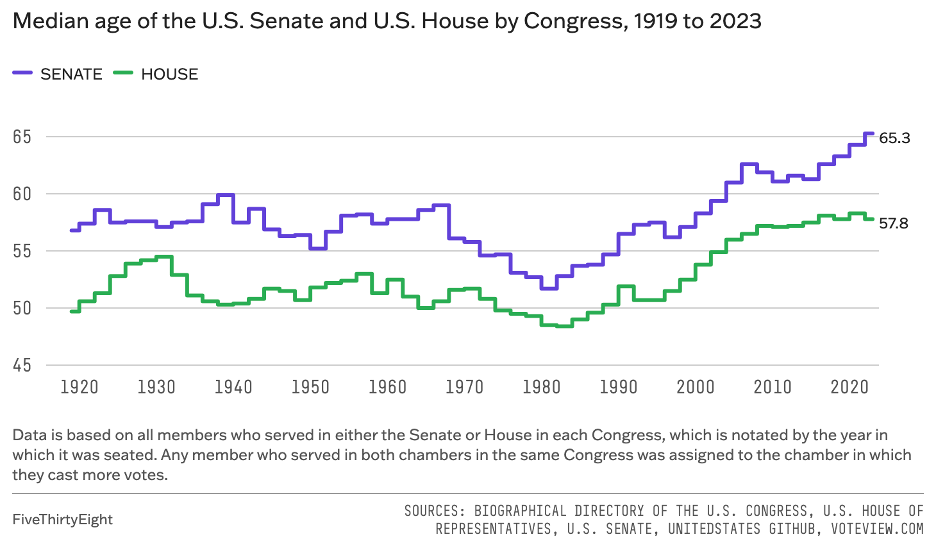
Over the past few years 50 years, the average age of our Senate has risen about a decade to 65 years old. The House of Representatives is younger than the Senate, but they’ve also gotten older in a similar fashion.
As a physician, I can’t help but see parallels between our government and our nation’s physician workforce.
When in doubt, choose the scarce resource
When I was choosing a specialty as a third-year medical student, I had diverse interests in emergency medicine, psychiatry, and urology. In the end, I chose urologic surgery, which covers a wide variety of medical conditions and cancers with treatment options ranging from medication to surgery.
In particular, I loved the prospect of using a literal laser beam to shatter stones within the kidney. When I saw demonstrations of this surgery, it looked like a fun video game to me. It’s still a favorite of mine to this day.
Another factor that led me to urology was simple supply and demand. In 2021, a national survey of urologists showed that the number of urologists in the country had increased to 13,790, which was a paltry 3% increase from 2015. Over that same time period, the nation’s population increased by 3.4%.
While these percentages aren’t terribly different, average Americans are steadily getting older, which means that the demand for specialty medical care is increasing as well.
Looking at these trends, I felt assured that my medical expertise would always be in high demand.
Urologists are aging faster than the country
The real ticking time bomb, however, is the average age of our nation’s urologists.
According to the American Urological Association, 50% of all urologists in 2021 were 55 years of age or older. What’s more striking, thirty percent of our nation’s urologists were already 65 years old at the time of the survey!
Given these numbers, it’s not surprising that the number of urologists per capita are declining (and are likely to continue to decline for the next 40 years).
In terms of the larger physician workforce, there has been a general acknowledgement that we are already in a physician shortage and that it’s going to get worse over the next decade. (I’ve covered this phenomenon in another article: The Physician Shortage: A Threat to the American Healthcare System.)
Already, about a third of our nation’s cities exist in medical deserts, with limited access to basic primary care physicians.
The average age of our physician workforce will be only contribute to this shortage, as the older generation of baby boomers seek retirement.
Our country’s worsening access to medical care has not gone unnoticed, with organizations like The Commonwealth Fund, a medical think tank that graded US Healthcare dead last amongst the top 10 wealthiest nations examined in its most recent examination.

When we start looking for solutions to the shortage, a few options emerge.
Keep them working!
One easy solution is to preserve our current workforce as long as possible. This can be done by minimizing both early and regular retirement, which will give us time to slowly increase the supply of new physicians.
You can envision a package of incentives to make this a reality. For example, there could be increased compensation offered to our older physicians to keep working past retirement age. Or perhaps there could be efforts made to improve the working conditions of this greying cohort, making their day-to-day work lives more pleasant.
But would this be effective? My own experience makes me very doubtful.
My experience as a Kaiser employee
When I worked for the Kaiser Permanente system in Southern California, one of the defining features of employment with the group was the mandatory retirement age. I knew that if I stuck with the medical group, when I turned 65 years old, I’d be forced to retire.
This wasn’t some autocratic rule from an ageist administrator at the top of the organization. The mandatory retirement policy was a popular provision approved by the physician group itself. Every once in a while, it came up for a vote and was reapproved with great support.
To be honest, I liked this feature of employment at Kaiser. As chief of my urology department for two years before I eventually left the organization, I received a special insight into the medical group.
Forced retirement?
When we discussed things like the forced retirement age, the conversation revolved around surprising factors.
One thing that wasn’t discussed was the issue of mental or physical competency. There was general acknowledgement that a 65-year-old physician could have many years of effective practice ahead of them if so desired.
(Just like it’s hard to know when someone is too old to serve as President, it’s also difficult to know when someone is too old to practice as a physician.)
But I clearly noticed a tacit understanding that being a physician is very demanding, and that all humans deserve at least some time at the end of their lives to enjoy their retirement.
It helped that Kaiser Permanente in Southern California is one of the few remaining organizations that offers a pension. This helped to greatly ameliorate usual worries related to income in retirement. I saw that the pension, as well as opportunities for part time work, freed the older physicians to make their retirement decisions from a place of financial security.
In my time with the organization, I saw some 65-year-old physicians move on from Kaiser employment to take another job elsewhere and continue their practice. But more often, I saw older physicians take the opportunity to actually retire for real.
Putting it all together
When I think of this experience and apply it to our nation’s physician workforce, I don’t think we will be too successful in keeping our doctors working endlessly past retirement age.
Instead, I believe most physicians will retire around the traditional age of retirement (or earlier, if they’re financially able to do so).
This choice likely won’t be made from physical necessity, as I believe most physicians can practice safely beyond the age of 65 years old. Instead, the choice to retire will center around a key part of the American Dream: that we all deserve some time to rest and enjoy ourselves before we die.
And while medicine has the potential to offer a high level of professional satisfaction, several trends in American healthcare are steadily eroding this perk. From generally high levels of burnout to ever-increasing frustration with the insurance industry, there is less and less idealistic love for the practice of medicine.
With Medicare reimbursement down about 30% over the last 20 years, you might argue that physicians will keep on working past retirement out of financial necessity. But doctors are smart. I talk to many of them when I wear my other hat as a founder of a real estate investment company.
By diversifying their income streams via investment and side gigs, our nation’s physicians are being proactive about their financial futures. I have confidence they’ll be financially prepared for retirement.
What do we do?
If our physician workforce is swiftly ageing and unlikely to continue to work until they keel over onto their computers, what do we do?
This is a topic of much debate with some clear potential solutions, such as increasing our use of midlevel providers and international physicians or increasing our number of residency training spots. The best strategy will likely include some combination of all three of these options.
If we look at the most recent data from my specialty, there’s some reason for optimism. In the journal “Urology”, a diverse group of researchers found that the total number of urologists from 2015 to 2022 has risen over sixteen percent. This reflects an increase in the number of residency training spots over that time.
As a side effect of the increased trainees, the average age of our nation’s urologists is falling slightly (from 55 to 54.5 years), reversing the trend. This is tremendously encouraging.
The authors expressed some concern, however, that this reassuring trend might be cancelled out by another interesting trend – a desire for earlier retirement. They noted “a decreasing age of planned retirement, from 68.91 to 67.70 years” in the study cohort.
On balance, we have some glimmers of hope that the medical profession is responding to the growing and already considerable need for medical care in the United States.
Whether or not it’s too little, too late, we’ll all find out together.
— Daniel Shin, MD
The Darwinian Doctor
If you’re a physician, when do you plan to retire? Let me know in the comments below!
Experience the financial benefits of real estate without dealing with the headache!
Want to support the blog?
- Join our investor club at Cereus Real Estate
- Visit my Recommendations page
- Check out my wife’s food blog: Eat Dessert First
- Check out my TikTok channel
- Follow me on Instagram
- Follow me on YouTube
- Contact me with questions


very good article! After 40+ yr in a solo ophthalmology practice in a small town., I am retiring in 1 month. I am the sole general ophthalmologist with the nearest ophthalmologist about an hour away. There is no one stepping up to take my place. I feel this is due to several reasons. 1. I never was able to recruit another ophthalmologist as I felt beefing up the numbers helped my bottom line but didn’t help my patients. Over the years I have seen patients coming to me because they felt their previous ophthalmologist did exams/ tests unacceptably often, which generated income but of no actual patient benefit. 2. I did comprehensive ophthalmology and not just procedures that generated higher reimbursement. Thus private equity companies were not interested. 3. New ophthalmologists are not interested in the intangible benefit of long term family relations but rather minimizing risks by taking a job with a larger practice. Conversations with other professionals reveal a lack of training in how to run a business( similar to dentistry and law schools)4.in my training I was taught to make decisions based solely on the patient’s benefit. It seems now that there has been a paradigm shift whereby if a specific treatment benefits the physician and does really”harm” the patient, then that is the best treatment. 5. It amazes me when after talking with a patient, they exclaim “ no one has ever explain that to me “ and “ no one ever took the time to speak with me for that long”. I realize these days, time is money , however taking time to explain something to a patient in a way they can understand provides empathy that seems lacking.
in summary, I’m not surprised that patients often don’t trust physicians and are dissatisfied with the current state of medicine with all our putting money before our patients.
Thank you so much for your perspective David! Congratulations on your 40+ year career. I hope you have a fantastic retirement and thank you for your many years of service to your community!